Could the stiffness in your neck be the cause or a contributing factor upper back pain?
We have your health, and the prevention of pain and impairment, in our best interest and priority. We have decided to write a blog post to provide you with information to help minimise your risk of developing a stiff spine, and therefore future pain and impairment that can occur soon after.
First we will explain the anatomy of the spine:
The spine is comprised of 32 individual bones (called vertebrae) stacked on top of one another and is divided into five parts:
- The Cervical spine: 7 stacked vertebrae which form the neck
- The Thoracic spine: 12 stacked vertebrae which support the chest and ribs
- The Lumbar spine: 5 vertebrae which form the lower back
- The Sacral spine: 5 fused segments which are attached the pelvis
- The Coccygeal spine: 5 fused segments which form the tailbone
As you can see from the image above, the spine naturally is formed with two types of curves – a concave curve (known as kyphosis) and convex curve (known as lordosis). The concave segments are located in the thoracic, sacral and coccygeal regions of the spine – hence the thoracic, sacral and coccygeal spines are kyphotic and the cervical and lumbar regions of the spine are lordotic. When these natural curvatures are lost, the muscles surrounding the joints can become shortened, tightened and/or weakened. This can result in further loss of the natural shape of the spine and eventually, pain.
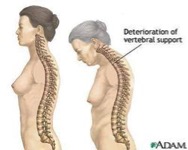
Certain activities in modern society cause us to hold abnormal postures for long periods of time for example, this could be standing looking at our phone, or sitting at a desk working on a computer. If we hold these positions long enough, loss of the natural curvature of our spine can occur and adaption of these odd positions can be adopted for the long term. This puts additional strain through spine. As you can see in the images of slouched postures, there is loss of the lumbar and cervical lordotic curvature and an increase in the thoracic kyphosis occurring.
Stiffness in the thoracic spine is a very common impairment. A specific syndrome that can develop with recurrent stiffness and build up of decreased movement of the thoracic and cervical spines is T4 syndrome.
An introduction to T4 syndrome
T4 syndrome develops as the stress on the spine from sustained postures specifically stresses the joints between the T3 and T4, and T4 and T5, vertebrae. T4 syndrome presents as the following symptoms:
- One or both hand glove-like pins and needles and/or numbness
- Aching, heavy limbs or neck region
- Sensations of limbs or neck feeling heavy, cold, or swollen
- Head aches
- Spasms of the surrounding musculature in the abdomen, or upper and middle back regions
- Popping sound and/or sensation the chest region
Poor posture and movement patterns can lead to:
- Winging of your shoulder blades
- Reduced ability to move your thoracic spine through extension (bending back) and rotation ranges (twisting side to side)
- Poor control of your lumbar (lower) spine so that you have difficulty tilting your pelvis anteriorly, further weakening your core musculature
- Poor movement patterns of the neck and shoulder
- Weak and/or tight surrounding musculature specifically middle and lower trapezius and serratus anterior (the muscle that holds your shoulder blades to your rib cage walls on your back)
Right-sided shoulder blade winging
This explains that although there are only two vertebrae of the spine implicated in this syndrome, the consequences of this stiffness can occur in other segments of the spine and in your limbs.
The physiotherapists here at Therapia provide many services which can help speed up your recovery when you start to experience pain and disability secondary to the development of stiff segments of your spine. These techniques will also help to prevent future episodes; they can be seen listed below:
- Manipulation and/or mobilisation of the stiff segment(s)
- Posture correction
- Correcting musculature imbalances: e.g. increase strength of deep neck flexors, middle and lower trapezius and serratus anterior and ease tension of potentially tight musculature including suboccipital extensors, upper trapezius, levator scapulae and the erector spinae
- Mobilising exercises
- Ergonomic advice
- Dry needling to the affected muscles and fascia
- Neural desensitisation through nerve mobilisations
The original question: “Could the stiffness in your neck be the cause or a contributing factor upper back pain?” Has been answered in this blog post. We have explained that the spine is a mobile, multidimensional structure connected by 32 vertebrae, and the effect of just one segment of the spine can influence all other areas.
Although every person is different and we highly recommend you come and see us at Therapia if you are presenting with the described symptoms, we have devised a home exercise program to prevent the development of stiff spinal segments, which can lead to the development of injury. Please understand no pain should be felt when performing the following exercises. Please see below:
1. Cervical flexion and extension – looking up and down (Figure 1)
- Look to the roof as far as possible, hold for 2 seconds and return to the centre
- Then look to your belly button touching your chin to your chest, hold for 2 seconds and return to the centre
Figure 1
2. Cervical rotation – looking to left and right (Figure 1)
- First ensure you have a good posture, maintaining the lordosis of your lumbar spine
- Look as far as possible to left, hold for 2 seconds and return to the centre
- Look as far as possible to the right, hold for 2 seconds and return to the centre
3. Thoracic extension (Figure 2)
Figure 2
- Sitting on a chair which has a high back
- Place a rolled towel horizontally behind your shoulder blades
- Place both hands behind your neck and interlock your fingers
- Touch elbows together
- Bend backward to a comfortable position and hold for 30seconds
- Perform 3 x daily
4. Thoracic rotation in side lye (figure 3)
Figure 3
- Lye on your side with your arms straightened at shoulder height
- Start to lift the top hand up and over to the opposite side of the body and onto the floor
- Make sure your thumb of the top hand remains in your sight at all times
- Your knees must stay together
- Your bottom shoulder should remain on the floor
- Hold for two seconds
- Return to the starting position
- Repeat 15 times on both sides
5. Prone cobra (Figure 4)
- Lying on your stomach
- Prop on to your elbows so that they are directly underneath your shoulders, let gravity drop your lumbar spine downwards, do not squeeze your glute muscles tightly
- Hold for 2 minutes
This entire routine should be performed twice daily.
The best treatment methods for T4 syndrome varies from person to person, as the causes of the syndrome vary significantly, for example the stiffness may have developed with an illness which included a constant cough as a symptom, a lifestyle change so that daily postures are modified e.g. increased sitting or decreased physical activity, or perhaps after a car accident in which trauma to the spine occurred. The evidence therefore is minimal as different techniques work differently for different people depending on their own personal causes and contributing factors. We here at Therapia want to really get to the cause of your symptoms and will use techniques based upon clinical experiences and best evidence.
The following articles contain information on the causes and treatment of T4 syndrome which further support the information included in our blog.
References
Conroy, JL. & Schneiders AG 2005, ‘The T4 syndrome’, Manual Therapy, vol. 10 no. 4, pp. 292-296.
DeFranca, GG & Levine, LJ 1995, ‘The T4 syndrome’, Journal of Manipulative Physiotherapy, vol. 18, no.1, pp. 34-37.
Evans, P 1997, ‘The T4 Syndrome: Some Basic Science Aspects’. Physiotherapy, vol. 83, no. 4, pp. 186-189.
McGuckin N, The T4 Syndrome, in Modern Manual Therapy of the vertebral column, G.P. Grieve, Editor 1986, Churchill Livingstone: Edinburgh. p. 370 – 376.
Mellick, GA. & Mellick, LB 2006, ‘Clinical presentation, quantitative sensory testing, and therapy of 2 patients with fourth thoracic syndrome’, Journal of Manipulative Physiotherapy, vol.. 29, no. 5, pp. 403-408.
Book Appointment